I’ve just realized that I’ve been a bit slow on the uptake. I’ve been aware of the results of the surveys of colds and flu in New York City carried out by scientists at Columbia University [1-3] for a few days without spotting that they’ve supplied a particularly important bit of evidence in the puzzle of explaining, properly, the seasonality of colds and flu.
Obviously we get fewer colds and flu bouts in the summer than in winter, and this seasonality of respiratory tract viruses (respvirs) is a controversial topic, with many different explanations being put forward. Scientific reviews of the evidence, however, generally admit that there’s no good explanation for it [4, 5]. The trend is almost universal, though. With one known exception (parainfluenza type 3) every viral illness that is mainly transmitted by coughing, sneezing and runny noses is less common in temperate regions in the summer months than in the colder seasons. This includes completely unrelated viruses such as adenovirus (a DNA virus), influenza (an RNA virus that replicates in the cell nucleus), measles, mumps, RSV (three RNA viruses that replicate in the cytoplasm) and coronavirus (unusually, a “positive-sense” RNA virus). We can’t really claim to understand respvirs unless we can explain their seasonality.
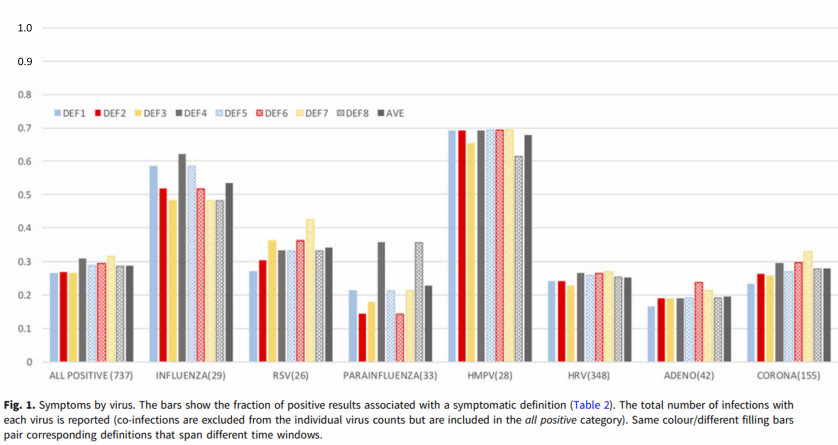
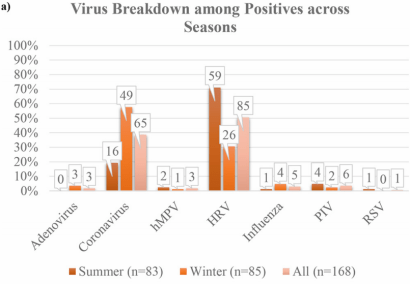
Four broad mechanisms have been put forward by scientists to explain seasonality. The first two, which I labelled M1 and M2 in my 2016 review in Medical Hypotheses, are about transmission. M1 says we tend to crowd together more in cold weather, while M2 says that the virus can survive outside the body for longer in winter. What the Columbia University studies showed was that (1) around 70% of infections by respiratory viruses were asymptomatic , and, crucially, (2) that as many respvirs were present in the noses and throats of participants in the summer as in the winter. In fact, the most common respvir, rhinovirus, was more than twice as common in summer than winter! Overall, the investigators found that “across time, between 10% and 25% of the samples tested positive each week, but this overall rate of positivity did not exhibit a trend or seasonality” [3].
It’s taken me a few days to realize the importance of the second result. If the virus is present all-the-year-round, very often in an asymptomatic form, then we can rule out M1 and M2 as the main drivers of seasonality. We don’t need to look for reasons why these viruses can spread more in winter than in summer – if, in general, they don’t! (Of course I’m not saying M1 and M2 have no effect, just that they’re not the main drivers of seasonality.) So now we need to focus only on mechanisms that can convert asymptomatic infections into symptomatic ones.
That leaves the last two possible drivers, M3 and M4. M3 says that our immune defenses in the respiratory tract are weaker in winter than in summer. This is a much better candidate. Two American doctors, Mudd and Grant, showed in 1919 that when someone is chilled, for example by putting a wet towel on their back, the blood supply to their tonsils and pharynx decreases and the temperatures at these sites drop within a few minutes [6]. It’s not that our immune systems overall function worse in winter than summer: a study showed that vaccination in winter is, if anything, slightly more effective than vaccination in summer. But there seems to be a specific effect of chilling on our respiratory tract defenses.
However there are two problems with M3 as a seasonal driver of respvir illnesses: firstly, chilling didn’t show up as a cause of colds in the many classical studies that were carried out the 1950s and 60s. These studies normally used a “pedigree” cold-virus strain. That’s to say, the investigators took “snot” from someone with a cold, and put it into the noses of volunteers who were paid to have “holidays” at their centers and participate in experiments. (Cold viruses had not been well-classified at the time of many of these experiments, and the scientists sometimes had little idea of exactly what virus they were using; presumably they used trial-and-error to make sure that the sample they were using was safe!) Some of the volunteers were chilled, others kept warm. Which treatment they underwent, however, had no significant effect on the chance of getting a cold. This was repeated in many labs and over many years.
Now if M3 has such a powerful effect that it can drive the near-universal winter seasonality of so many respvirs, why didn’t it show up in these classical experiments?
The second reason that I’m skeptical of M3 – as a major seasonal driver – is that colds and flu are common year-round in the Tropics, much more common than in Europe and the USA at mid-summer. If our immune defenses work well during the summer here, why don’t they work in the Tropics where people are presumably less likely to be chilled?
That leaves M4, which I’ve proposed as the main driver of seasonality. I suggest that respvirs need a good way to stay in the nose and throat of their hosts, and to keep out of the lungs, heart, brain etc. If they go down into the lungs etc, they’re likely to make their host very sick, and – disastrously from their point of view – stop him or her from moving around and meeting other potential hosts. We usually stay at home and go to bed if we get fevers or muscle aches. Virtually all respvirs seem to have solved this problem in the same way: they’ve developed temperature-sensitivity. They replicate at temperatures below normal body-temperature, which normally means the nose and throat, and they become inactive at the higher temperatures of the lungs and other organs. Seasonality is, I suggest, a side-effect of this mechanism. As ambient temperatures increase in spring, the temperatures in the nose and throat also increase. The viruses then become less active, and we get fewer colds and bouts of flu. When fall arrives, and then winter, the temperatures in the nose and throat decrease as we breathe in the colder air. Now the virus becomes more active – so active that it may “accidentally” move down into the lower respiratory tract and cause fevers, possibly even getting into the blood-stream. This explanation, the TDVT hypothesis, is described in other posts in this blog.
Covid-19 has recently jumped into the human species from another animal. Therefore it’s not optimized to its host, and may not have much temperature-sensitivity when compared to well-established human respvirs. In practice, it seems to have retained some temperature-sensitivity because it often confines itself to the nose and throat, and also settles in the toes (causing chilblains). Like the nose and throat, the toes are some of the coldest parts of the body. Exactly how temperature-sensitive the virus is would be a very good subject for some urgent lab-work.
Patrick Shaw Stewart, 8 May 2020.
For more thoughts on the Columbia University study click here.
[1] Galanti, M., et al. “Rates of asymptomatic respiratory virus infection across age groups.” Epidemiology & Infection 147 (2019).
[2] Birger, Ruthie, et al. “Asymptomatic shedding of respiratory virus among an ambulatory population across seasons.” mSphere 3.4 (2018): e00249-18.
[3] Galanti, Marta, et al. “Longitudinal active sampling for respiratory viral infections across age groups.” Influenza and Other Respiratory Viruses 13.3 (2019): 226-232.
[4] Tamerius, James, et al. “Global influenza seasonality: reconciling patterns across temperate and tropical regions.” Environmental health perspectives 119.4 (2011): 439-445.
[5] Dowell, Scott F., and Mei Shang Ho. “Seasonality of infectious diseases and severe acute respiratory syndrome–what we don’t know can hurt us.” The Lancet infectious diseases 4.11 (2004): 704-708.
[6] Mudd, S., and S. Grant. “An experimental study of a possible mechanism for the excitation of infections of the pharynx and tonsil.” Am J Physiol 49 (1919): 144-145.
_____________________
The TDVT Hypothesis, as explained by my friend Brian.
For a general discussion of the seasonality of respiratory viruses, written for the layperson, please see Every winter, colds and flu increase.

One thought on “Another piece of the respvir seasonality jigsaw falls into place”